The airway is composed of the upper and lower jaws, tongue, tonsils, soft palate, and side wall of the throat. Different surgical procedures in the treatment of OSA have been developed to address these different components of the airway. Because the airway pattern and the severity of obstruction vary greatly between individuals, the success rate of a given surgical procedure also varies greatly. In general, as the severity of OSA increases, so does the invasiveness of the required procedures in order to achieve successful surgical outcomes.
Nasal Surgery Treatment Course:
Domestic patients require a total of 2 week stay in the area
International patients require a total of 3 week stay in the area
Preoperative requirement:
Avoid Aspirin or Ibuprofen for at least 7 days before surgery
Covid Test 24–48 hours prior to surgery
Intraoperative and hospital course:
Surgery duration is approximately 1 hour under general anesthesia
Hospitalization is typically not required
A nasal splint is placed in the nose at the end of the operation and is to be removed by Dr Li the following day
Postoperative management:
Sleep with head elevated (two pillows so the head is above the heart)
No nose blowing for at least 7 days
Some bleeding from the nose is normal the night of the operation. It is important to change the gauze at the front of the nose when it is soaked with blood or mucus
OTC pain medication such as Aspirin, Ibuprofen or Tylenol can be used if pain is not severe
If pain is significant, Hydrocodone can be used (prescribed by Dr. Li)
Pain control consists of Hydrocodone every 4 hours
No exercise for 10 days but walking is encouraged starting post-surgery day 1
Liquid or soft food diet for the night of the operation and normal diet can be resumed the day after the operation
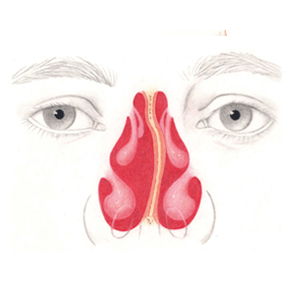
Before
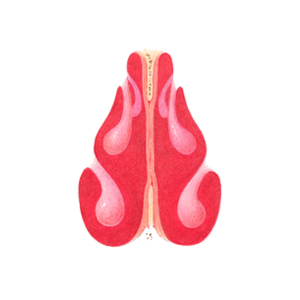
After
References:
Li KK, Powell NB, Riley RW, Troell RJ, Guilleminault C. Radiofrequency Volumetric Tissue Reduction for Treatment of Turbinate Hypertrophy – A Pilot Study. Otolaryngology – Head and Neck Surgery; 119(6) 569-573, 1998.
Troell RJ, Powell NB, Riley RW, Li KK. Evaluation of a New Procedure for Nasal Alar Rim and Valve Collapse: Nasal Alar Rim Reconstruction. Otolaryngology – Head and Neck Surgery; 122(2):204-211, 2000.
Guilleminault C, Kim Y, Palombini L, Li K, Powell N. Upper Airway Resistance Syndrome and its Treatment. Sleep; 23:S197-S200, 2000.
Powell NB, Zonato A, Weaver EM, Li K, Troell R, Riley RW, Guilleminault C. Radiofrequency Treatment of Turbinate Hypertrophy in Subjects Using CPAP. A Randomized Double Blind Placebo-Controlled Clinical Pilot Trial. Laryngoscope; 111:1783-1790, 2001.
Li KK, Powell NB, Riley RW, Troell, RJ. Radiofrequency Volumetric Reduction for Turbinate Hypertrophy. Operative Technique of Otolaryngology-Head and Neck Surgery; 11(1);24-25, 2000.
Li KK, Powell N, Riley R. Radiofrequency Thermal Ablation Therapy for Obstructive Sleep Apnea. Oral and Maxillofacial Surgery Clinics of North America; 14:359-363, 2002.